Impending Legislation in the UK from a viewpoint of a peer-led support group. Picking up the pieces regardless of the law.
1.0 Context
Cannabis is the most widely-used illegal drug in Britain.
According to the Statistics on Drug Misuse: England, 2018, 6.6% of adults 16-59 reported having smoked cannabis in the last year.
29% of adults have smoked cannabis at least once in their life (EU average 26%).
Among younger adults aged 11-15, cannabis was also the most commonly used drug,
with 8% having admitted using it in the preceding year.
2.0 Introduction
In view of recent cuts in services, the recovery resources available to current and former drug users have been further squeezed. [REF-001] Most commissioners and providers have reverted to a ‘fire-fighting’ model of greater harm/crime reduction which naturally has prioritised users of heroin and crack to the detriment of all other service users. Buoyed by legislative developments in US states – where evidence suggested that even violent crime had been reduced as a consequence of cannabis legalisation [REF-002]– and the development of medical CBD markets, cannabis users in particular have been pushed even further down the list of priorities as cannabis use perception switches away from a harmful illegal drug towards a society preparing for possible legalisation. This, coupled with the wider belief that cannabis is a soft drug, with no physical dependency, does not fit into the bracket of a problematic drug [REF-003]. This view is present not only within the drug-using community, but in wider society and even some parts of addiction services.
2.1 The three strands:
(1) Increased THC content/reduced CBD content.
(2) Lack of understanding/recognition of cannabis as a problematic drug.
(3) Reduced resources and priorities as part of wider austerity cuts.
Combine to exacerbate the cannabis misuse crisis that is present in UK society.
Presently there is no evidence to suggest a physical addiction, however, there is a universally recognised condition of psychological dependency. In addition, there is Cannabis Use Disorder, documented in DSM-5 below:
2.2 The Problem Area
2.2.1 DSM-5 Definition of Cannabis Use Disorder
- Cannabis is often taken in larger amounts or over a longer period than was intended.
- There is a persistent desire or unsuccessful efforts to cut down or control cannabis use.
- A great deal of time is spent in activities necessary to obtain cannabis, consume cannabis, or recover from its effects.
- Important social, occupational, or recreational activities are given up or reduced because of cannabis consumption.
- Cannabis consumption is continued despite knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by cannabis.
- Tolerance, as defined by either a need for markedly increased cannabis to achieve intoxication or a desired effect or a markedly diminished effect with continued consumption of the same amount of the substance.
- Withdrawal, as manifested by either the characteristic withdrawal syndrome for cannabis or cannabis is taken to relieve or avoid withdrawal symptoms.
2.2.2 Reality
Despite the widely held view that cannabis is not a problematic drug, significantly more users are presenting at services citing cannabis as a drug that creates serious issues affecting their relationships, lifestyle, career, and mental health [REF-004]. The reasons for this are multiple and complex. Firstly, it may be argued that traditional services are now well established, accessible, and better-known to the using community, particularly in an aging, experienced, media savvy drug-using population. Secondly, users who have addressed and managed an opiate addiction, for example, may still be using cannabis and alcohol to help maintain their drug of choice recovery. They may, however, continue to be locked into a routine of cannabis use that is becoming more frequent, stronger, and increasingly problematic. Finally, and perhaps more significantly, the nature of cannabis production has changed over the past 30 years to include a higher THC content whilst containing lower CBD levels. [REF-005] With CBD showing evidence of mitigating psychotic tendencies of THC [REF-006] its absence from street cannabis may account for increasing problematic use. Furthermore, anecdotal evidence suggests untested chemical compounds are increasingly used in the domestic growing process to enhance growing/flowering with the aim of increasing potency and yield. The result of these stronger cannabis strains has manifested in more presentations of mental health problems such as: psychosis, paranoia, depression, and schizophrenia. [REF-007]
2.2.3 Services
To further compound the issues facing problematic cannabis users, individuals seeking help with their cannabis misuse are less likely to engage with traditional services. The Adult Psychiatric Morbidity Survey reports 36.2% of drug users dependent on drugs other than cannabis have received treatment, help, or advice, whereas users of cannabis were half as likely to have received the same support. [REF-003] Reasons for this are steeped in perceptions of drug treatment centres and are engulfed in widely held beliefs between users concerning drug use hierarchy and stigma. Firstly, cannabis users are less likely to see their drug use as problematic or dependent and are more likely to see users of other (harder) drugs as suffering from addiction and having nothing in common with their drug of choice. Again, this is reinforced through widely-held beliefs in the greater (non-drug using) population, including some traditional services. [REF-004]
Cannabis users do display many symptoms and issues that they have in common with other substance users. Issues such as heightened anxiety and paranoia may be shared with stimulant users, whereas Issues of isolation and withdrawal from society may be shared with depressant users. Similarly, cannabis users may, like abusers of alcohol, come under tremendous social pressures in an environment of acceptance and normalisation. Cannabis users do however have a set of unique circumstances unlike other addictions.
The single issue of isolation and the general withdrawal from society makes problematic cannabis use less visible. Cannabis users are less likely to commit crime or become violent [REF-008] than other substance users and as such reduces the visibility of problematic use. Similarly, hospitalisation and medical intervention is not likely to occur until after many years of problematic use [REF-009] Also, the production and distribution of cannabis is well established in the UK and is not limited to geographical areas.
In user-led self-help groups such as The Cannabis, Spice & Legal Highs Group, attendees report a reluctance to engage with traditional services. More so there is also initial resistance to attending other mutual aid groups such as Narcotics Anonymous (NA) and Self-Management Recovery Training (SMART) for the same reasons stated earlier of not wanting to mix with ‘hardened’ drug users. This distancing of cannabis users from the wider recovery community is a consequence of the specific characteristics of frequent and prolonged cannabis use. Problematic cannabis users are more likely to suffer from isolation, paranoia and depression and as a result are more likely to avoid larger social gatherings. Within Cannabis, Spice & Legal Highs Group meetings, attendees often have a preliminary view that they are suffering alone and that their symptoms and frustrations are unique.
2.2.4 Disclaimer
Before outlining possible solutions, it must be pointed out that there is no universal fix or ‘one size fits all’ solution. Since each cannabis user (like all substance users) began their own addiction from a unique and individual set of circumstances, their exit from addiction will be equally unique. More importantly, individuals need to define their own recovery based on their own experience and taking responsibility for a path and pace that works best for them. There is a misplaced view in recovering addicts that conflates progression with knowledge and perceived wisdom. There is also a desire to ‘give service’ and help others but without appropriate maturity this can manifest as advice given in comments such as: ‘what worked for me, will work for you’. It is common to hear recovering addicts advising those newer to recovery with ‘you should or shouldn’t do this or that’. This approach is not always helpful, worse still it can further isolate newcomers who may have had to overcome anxiety and stress to make it to the meeting in the first place.
2.3 Solutions
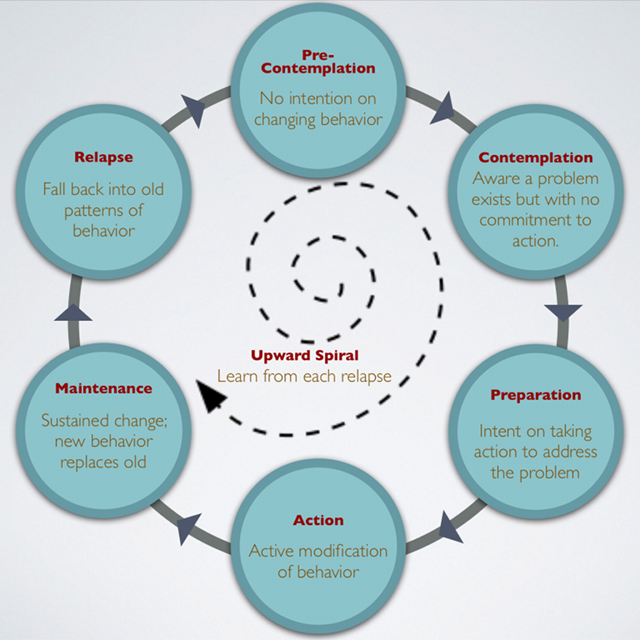
In order to get help, cannabis users have to be identified and offered realistic pathways into recovery. As is often the case with an aging drug-using population, word of mouth and personal referral is often the key. The vast majority of the illicit drug trade relies on an absence of marketing and thus a word of mouth culture persists, driving functionality where information on drugs and drug dealers is communicated socially. Friends often introduce a drug culture to a peer group and recovery is no exception. In the same way, one member of a social group may enter recovery and others may follow. They may act as a pathway to services and abstinence by example. This phenomenon also conforms to a cycle of drug use that is particularly prevalent where addictions last over 20 years. Users in this cohort rarely use as a result of the motivations and circumstances that originally got them into drug taking in the first place. Following this, a process of sick and tired of being sick and tired [REF-010] becomes to take hold. Such users at the end of their addiction begin to research and enquire possible pathways to recovery [Fig-1-Cycle of Change]. However, without clear guidelines, pathways, and examples of peers who have been through recovery, it is difficult for the addict who is ready for change to access traditional services and support. GP practices are often the first option but can often prove ineffective. There is also a real fear of lack of confidentiality, inadequate knowledge, a poor experience of the issues, and an absence of a practical treatment-based solution for cannabis rehabilitation.
More often than not, cannabis users are unaware of available help. Most peer examples of abstinence are achieved as individual efforts. Users of other drugs, like heroin and crack, may present at services as a result of an intervention such as a criminal conviction or hospital admission. However, with even chronic cannabis users, this is statistically less likely. Only recently has cannabis support provision been identified as a result of increased presentations. [REF-005]
Forward-looking organisations such as The Bridge Project in Bradford have been frontrunners in highlighting the increasing dangers of cannabis misuse: both traditional, contemporary, and synthetic. It was from this concern and knowledge that the Cannabis, Spice & Legal Highs Group was formed as a collaboration between Bridge practitioners and service users in March of 2015. The group offers peer-led, non-judgemental advice and information in mutual aid meetings in local venues. To date, over 200 individual users have attended meetings and events, with over 729 instances of attendance in 2017. [REF-0011]
The recent rise in synthetic cannabis, specifically the advent of spice (the so-called ‘zombie drug’), is perhaps a precursor to the future development of street cannabis with particular reference to increased potency, not necessarily by increasing THC but by the introduction of more unknown and untested psychoactive compounds. Additionally, a real risk of the addition of psychoactive substances to street cannabis is statistically likely if anecdotal evidence of fentanyl added to street heroin [REF-012] is considered as a president. Dealers are more likely to put increasing potency as a factor in highlighting their product before any medium or long-term health risks.
It could be argued that legalisation may address this issue of THC/CBD ratios where evidence has been shown that higher ratios of THC produce an increased risk of dependence, memory impairment, and psychosis. [REF-013] With a regulated market comes the opportunities to apply a uniform quality benchmark that includes an increased CBD content that will not affect the users experience but includes mitigating anti-psychotic properties [REF-006].
In addition, other benefits to legalisation include the decriminalisation of users and the control of criminal involvement in production, distribution, and significantly in terms of financial gain. Moreover, the increased state revenues through taxation and licensing can be re-invested into addiction services, education, and better research. Such measures also are likely to lead to a reduced burden on police, emergency services, the NHS, and mental health services.
Caution should accompany any talk of legalisation. As previously stated there are no ‘silver bullet’ solutions. As a comparison, UK alcohol legislation, in practise, can hardly be viewed as a success story. Legalisation of alcohol has done little to reduce alcohol abuse, despite education campaigns, voluntary industry codes, and changes to licencing laws. If cannabis was to mirror alcohol’s path in terms of delivery and outcome, the UK will find its population firmly rooted to the top of misuse league tables and having to deal with all the associated problems and resulting costs. Cannabis legislation is currently less harmful as an illicit controlled drug than a rushed, ill-thought-out piece of legislation with only a verisimilitude approach to the underlying issues. In short, the harms of a poorly conceived and executed cannabis legalisation programme could be more damaging than the current status quo. This is an example where no deal really would be better than a bad deal.
2.3.1 A deeper look at Legalisation
Any effective cannabis legalisation programme would have to address the following issues:
2.3.2 Control
In order to take control out of the hands of criminal gangs, the state would have to seize the production and distribution of cannabis. The current free market in alcoholic beverages of (private) licenced premises is expensive and failing. A more effective solution would be to put the means of production and distribution in a state monopoly, at least initially, in a similar model to Sweden’s state-run monopoly on alcohol. The Systembolaget (The System) is a government-owned chain of off licences that are the only licenced retail store allowed to sell alcohol in Sweden. [REF-014] Any UK government advocating such state monopoly control would receive opposition, particularly from commercial interests that may wish (and are currently planning) to capitalise on such a scenario. However, particularly in the early years of a legislation change, overall control is essential in order for the programme to work. A correctly administered state-controlled distribution system could also comprehensively monitor and control consumption and quality. There may well be good reason to slowly turn the process over to commercial interests in the future, but only after a sustained period of stability and under strictly enforced guidelines.
2.3.3 Treatment
As with alcohol, or any drug, a certain proportion of the population, perhaps up to 10%, will misuse drugs regardless of the legal status. An effective network of drug addiction services must be adequately funded to deliver front-line services. This can be funded directly through distribution profits. Furthermore, state profits from legal cannabis sales could be re-invested into other substance misuse treatment programmes. The promotion of realistic recovery and effective treatment within a framework of un-stigmatised drug association will only work well in adequately funded, resourced and supported services, unlike the current status of drug and alcohol services.
2.3.4 Research
A criticism of current academic and scientific research is the lack of transparency and accessibility. To a certain extent, such reluctance to share information and practice also exists within traditional addiction services. [REF-015] As part of a cannabis legalisation programme, research would be adequately funded and charities and community groups should be encouraged to research wider aspects of cannabis use. Results and findings must be communicated in the wider population through: community, school, college, university, and media networks. In particular, an investigation into possible medical benefits suffers from a comprehensive qualitative and quantitative research policy. A wider funded approach would produce more effective investigation, particularly where known benefits have been highlighted in areas such as: pain relief, multiple sclerosis, arthritis, and certain cancer treatments.
2.3.5 Education
Again, using UK alcohol legislation and policy as a comparison of how not to handle a change in statute direction, education must be at the heart of any potential policy. The damage cannabis can do to the young-developing brain has been well documented. [REF-016] Applying a minimum consumption age for legal cannabis is unavoidable and by the same measure will inevitably lead to some adolescents using cannabis regardless of the law. Only a comprehensive education programme from an early age can reduce the danger of damage in young-developing brains. The unpopular but effective measure of testing under-18s for cannabis consumption would help to monitor, control, and enforce an age-related ban on legally available cannabis.
2.3.6 Enforcement
In order to maintain an effective embargo on non-legal cannabis, the law would have to be actively used in closing down what is in the UK: an advanced domestic growers market. The proliferation of cannabis farms is more likely to become less numerous as new legislation would price criminal gangs out of the illicit market in search of greater profits elsewhere. Individual homegrown crops, however, could prove more persistent due to the isolated nature of numerous individual grows. A better regulation of the home-grow sector, hydroponics and sodium lighting distribution, including the import and sale of nutrients, would help to further control this sector. The state would also have to rigorously enforce testing particularly in the areas of transport, youth, the workplace, and prisons. Any detection of drug misuse, illicit drug or otherwise, must be met with a comprehensive treatment and education programme.
2.3.7 Pricing
The unit cost and pricing structure of a legally available product will always be in direct competition with the criminal market. If legal cannabis becomes overpriced, the illegal market will naturally prevail. The factors of quality and availability are secondary to fundamental pricing. This again reiterates state involvement. Even beyond a state monopoly the government must have the authority to set the price of cannabis. The alternative is clear to see even in the regulated pharmaceutical sector, where drug prices can spiral out of control in a race for profit. There may be evidence to underprice the market initially in order drive out the criminal sector.
2.3.8 Delivery
By taking control of the cannabis market, the state would be able to re-think the process of delivery. In terms of viewing delivery in a harm-reduction context, the distancing of smoking as a delivery method must be a priority. The development of other delivery systems such as ingestion by edible products, nasal and oral sprays, patches, and beverages should be developed and encouraged as a healthier alternative to smoking which, has proven links to increased risk with nicotine dependence displaying clear associations to cannabis use disorder symptom [REF-017]. The opportunity for controlling tobacco consumption as a health choice can also be incorporated into cannabis legislation solutions.
2.3.9 Medical Cannabis/Recreational Use
Within the context of legalisation a clear distinction must be established from the onset to distance genuine medical users from problematic recreational use. Specifically, the following areas with regard to screening need to be addressed: [REF-018]:
(1) Existing cannabis screening tools may not be equally valid across medical and recreational users.
(2) Individual screening items may have different implications for recreational and medical users.
(3) There is a need to develop and validate criteria for problematic use in medical cannabis patients.
(4) Finally, the prescription of medical cannabis must follow strict clinical guidelines with caution regarding dependency and misuse.
To some extent it is the medical cannabis sector that the state must regulate the most. Pharmaceutical corporation lobby groups will be keen to exploit any legislation change and immense pressure will be put on legislation designers to appease commercial interests, this must not be to the detriment of greater potential benefit to the overall cannabis market.
2.3.10 Micro Economy
Most issues of state revenue (through taxation) result due to a change in legislation that will require careful consideration and planning in order to support the implementation of drug policy as largely described previously. The issue of local economic factors must also be addressed. The presence of money from the local cannabis market is not inconsiderate. We must accept the reality of drug markets and illicit revenue on local communities and its absence if the market is successfully regulated. Local growers and dealers are responsible for injecting revenue, employment and investment in to certain communities and some fragile economies may suffer adverse effects of legalisation that have not been fully considered.
2.3.11 Review
The issue surrounding UK legalisation has never been closer to a realistic possibility than it is today. Examples of European and US states have led the way in sea changes in the law. Feedback is ongoing and dynamic. It is imperative to monitor progress and consequence, adapting legislation and its approach accordingly. Controlling the cannabis market, would impact the wider drugs community. It is not uncommon for users of harder drugs to finance their addiction by selling cannabis. The advent of legalisation and state dominance of the cannabis market would close this revenue stream, resulting in severe impact to users of other drugs. Any care and treatment policy would need to react to such implications. By dominating the market, influence, and manipulation can affect potency, availability, frequency of use, choice, impact, and perceptions of drug use – none of which the state has effective influence over at the moment.
2.4 Conclusions
The imminent arrival of a change in cannabis legislation is more likely now than at any point within the past 50 years. Only in recent years has UK society begun to seriously consider and debate practical and workable scenarios and consequences. A real opportunity exists to tackle substance misuse in the wider sense. Specifically, evidence exists to suggest the likelihood of impacting tobacco and alcohol consumption, the latter of which may mirror outcomes identified in recent studies in the US where the relationship between alcohol and marijuana use was found to be decreasing since the passing of legalisation of cannabis [REF-019].
Undoubtedly, the greatest risk to cannabis legalisation lies with potentially increasing harm to youth. Both policy and legislation must be crafted carefully to incorporate opportunities for youth to self-refer to cannabis support [REF-020].
Despite the fact that, largely, the desire for legalisation is driven by (private) economic benefit motivations [REF-021], the temptation to loosely regulate the market must be resisted to enable the state to control and dominate the cannabis market in its entirety.
Cannabis, Spice & Legal Highs Group
https://www.cslhg.org
M. 07821 946 883
E. cslhginfo@gmail.com
Twitter: @cslhginfo
Facebook: fb.me/cslhg
3.0 References
[001]
“Cuts to Addiction Services Since 2010 [INFOGRAPHIC]”
Cassiobury Court
https://www.cassioburycourt.com/article/102/cuts-to-addiction-services-since-2010-[infographic]
[002]
“Is Legal Pot Crippling Mexican Drug Trafficking Organizations?
The Effect of Medical Marijuana Laws on US Crime” – (December 27, 2014). – Gavrilova, Evelina and Kamada, Takuma and Zoutman, Floris.
https://ssrn.com/abstract=2350101http://dx.doi.org/10.2139/ssrn.2350101
[003]
“Highways and Buyways: A snapshot of UK drug scenes”
Drugwise. 2016- Sharpio, H. Daly, M.
http://www.drugwise.org.uk/wp-content/uploads/Highwaysandbyways.pdf
[004]
Cuts to addiction services are a false economy
The BMJ Opinion- May 25, 2017- Colin Drummond.
http://blogs.bmj.com/bmj/2017/05/25/colin-drummond-cuts-to-addiction-services-in-england-are-a-false-economy/
[005]
“Why did cannabis treatment presentations rise in England from 2004/05 to 2013/14?”
Drug and Alcohol Today. 17(4). 2017′ -McCulloch, E.
https://www.researchgate.net/publication/320535752_Why_did_cannabis_treatment_presentations_rise_in_England_from_200405_to_201314
[006]
“Can we make Cannabis safer?” Lancet Psychiatry. 2017.
Englund, A. Freeman, T. Murray, R. McGuire, P.
http://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(17)30075-5/fulltext?elsca1=tlpr
[007]
“Statistics on drug misuse, England” NHS. 2017’
https://www.gov.uk/government/statistics/statistics-on-drug-misuse-england-2017
[008]
Predictors of violence in young tourists: a comparative study of British, German and Spanish holidaymakers Hughes K et al.
European Journal of Public Health, 2008, 18:569-574
[009]
Hospitalizations Related to Drug Abuse
Cheryl A. Kassed, Ph.D., Katharine R. Levit, and Megan M. Hambrick, M.S.W.
2005- Statistical Brief #39. Healthcare Cost and Utilization Project (HCUP). May 2008. Agency for Healthcare Research and Quality, Rockville, MD.
www.hcup-us.ahrq.gov/reports/statbriefs/sb39.jsp
[010]
21st Century Research on Drugs and Ethnicity: Studies Supported by the National Institute on Drug Abuse -P19, P24, P29-31 Peter L. Myers
https://books.google.co.uk/books?id=OjxpAwAAQBAJ&pg=PA29&lpg=PA29&dq=sick+and+tired+of+being+sick+and+tired++drugs&source=bl&ots=WPMt8HWVWi&sig=gfxX2Pnq8HAkQCLQ62gpwq7knBM&hl=en&sa=X&ved=0ahUKEwj62fHZzZjZAhULW8AKHaMGBUQQ6AEIZjAN#v=onepage&q=sick%20and%20tired%20of%20being%20sick%20and%20tired%20%20drugs&f=false
[011]
Cannabis, Spice and Legal Highs Group – Report 2017 -Attendance data
https://docs.wixstatic.com/ugd/6914c2_bc1bb7915e9245c396c0f61bc0811061.pdf
[012]
Is There a Relationship Between Street Heroin Purity and Drug‐Related Emergencies and/or Drug‐Related Deaths? An Analysis from Vienna, Austria
The Journal of Forensic Sciences- Volume 52, Issue 5. September 2007 -Pages 1171–1176
Daniele Risser M.D., Alfred Uhl Ph.D., Felicitas Oberndorfer M.D., Selma Hönigschnabl M.D., Martin Stichenwirth M.D., Robert Hirz Ph.D., Dieter Sebald M.D.
http://onlinelibrary.wiley.com/doi/10.1111/j.1556-4029.2007.00507.x/full
[013]
The Tide Effect -How the World is Changing its Mind on Cannabis Legalisation- Boris Starling
Plotting Changes -Volteface Journal Issue 01-p10
http://volteface.me/volteface-publish-first-journal-plotting-change/
[014]
Systembolaget
https://en.wikipedia.org/wiki/Systembolaget
[015]
Black Sheep- Lizzie McCulloch
Plotting Changes -Volteface Journal Issue 01-p118
http://volteface.me/volteface-publish-first-journal-plotting-change/
[016]
Effects of Cannabis on the Adolescent Brain
Current Pharmaceutical Design- Volume 20, Issue 13, 2014
Joanna Jacobus, Susan F. Tapert.
http://www.eurekaselect.com/111820/article
[017]
Nicotine dependence predicts cannabis use disorder symptoms among adolescents and young adults
Lisa Dierkera, Jessica Braymillerb, Jennifer Rosea, Renee Goodwinc,, Arielle Selyae
Drug and Alcohol Dependence. 16 April 2018
https://doi.org/10.1016/j.drugalcdep.2018.02.037
[018]
Rethinking indicators of problematic cannabis use in the era of medical cannabis legalization
Sharon R.Sznitmana, Robin Room
Addictive Behaviors, Volume 77, 2018, Pages 100-101, ISSN 0306-4603,
https://doi.org/10.1016/j.addbeh.2017.09.026
[019]
The impact of the legalization of recreational marijuana on college students
Jacob Jones, K.Nicole Jones, Jenny Peil
Addictive Behaviors, Volume 77, February 2018, Pages 255-259
https://doi.org/10.1016/j.addbeh.2017.08.015
[020]
Legalization of cannabis: Considerations for intervening with adolescent consumers
Denise D.Walker
Preventive Medicine, Volume 104, November 2017, Pages 37-39
https://doi.org/10.1016/j.ypmed.2017.07.010
[021]
Public perceptions of arguments supporting and opposing recreational marijuana legalization
Emma E.McGinty, Jeff Niederdepped, KathrynHeley, Colleen L.Barry
Preventive Medicine, Volume 99, June 2017, Pages 80-86
https://doi.org/10.1016/j.ypmed.2017.01.024
[Fig-1-Cycle of Change]














{kind=link}